
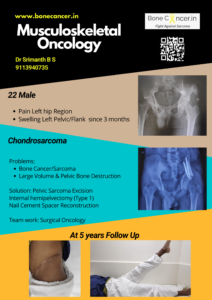
Chondrosarcoma
Signs | Symptoms | Treatment
Chondrosarcoma is a group of cartilage matrix producing tumors.
It is the third most common primary bone sarcoma.
It most commonly affects age group 30 – 60 years.
They grow very slowly and rarely have distant metastasis or local recurrence (15-25 %).
Etiology
- Etiology of chondrosarcoma (primary) is unknown.
- Exostosin genes (EXT 1 & EXT 2) have been identified in conventional chondrosarcoma, but of unknown significance.
- They can occur Primary (De novo) or Secondary (as sarcomatous changes in pre existing osteochondromatosis and enchondroma).
Location
- Diaphysis and Metaphysis of Long bones, pelvis and rarely spine
How is chondrosarcoma identified?
- An individual with Chondrosarcoma presents with dull pain and small palpable tender mass
- A preexisting mass (Exostosis) which has rapidly grown in case of peripheral chondrosarcoma.
- A successive physical, radiological examination is carried out including plain radiographs, MRI or CT scan followed by Biopsy (Needle).
- A PET CT is performed to obtain an idea on activity and complete staging.
In some situations a A PET CT guided Biopsy is performed to obtain the most active component of disease.


What are the different types & grades of chondrosarcoma?
- Different types of chondrosarcoma are
- Conventional (85 %, includes central, peripheral and juxtacortical based on location)
- Dedifferentiated (10%)
- Mesenchymal (<2 %) and
- Clear cell (< 2 %)
- Central chondrosarcoma are almost always Primary
- Peripheral chondrosarcoma are almost always secondary in origin.
Peripheral chondrosarcoma are actually secondary changes in cartilage cap of osteochondroma which is present for a long time (this statement does not necessarily indicate that all osteochondromas need to be surgically removed fearing malignant transformation).
- Different grades of Conventional chondrosarcoma are identified which is crucial for treatment and resultant survival.
- Grade I (Low Grade Chondrsarcoma) have low cell load and rarely metastasize (< 5 %) with survival rate of 83 %.
These are now termed as ACT (atypical Cartilaginous tumours)
- Grade II and Grade III are considered high grade with high chance to metastasize and have local recurrences in nearly 60-70 % individuals with survival rate of 64 & and 30 % respectively at 10 years.
- Grade IV is sometimes referred to as Dedifferentiated variety with pleomorphism and multiple cell lineages.
- Dedifferentiated chondrosarcoma is a very high grade tumor most commonly seen in pelvis and femur with rapid progression and metastasis, hence associated with bad prognosis (survival rate of 28 % at 10 years).
Chemotherapy and high doses (> 60 Cgy) of radiotherapy are the adjuvant therapies that can be attempted, but survival has not improved.
- Mesenchymal chondrosarcoma is also a high grade variety of chondrosarcoma which in addition to bone can occur in soft tissues also.
No specific etiology has been found.
But it has been recently identified to respond to a certain high intensity chemotherapy regimen and radiotherapy thereby increasing survival rate to 89 % at 10 years.
- Clear cell chondrosarcoma is a low grade variant commonly found in epiphysis of proximal femur, proximal humerus and proximal tibia.
Metastasis and local recurrences are very rare but require long term follow up (even upto 25-30 years) and the results are excellent.
- Of note, Myxoid chondrosarcoma is a different entity occurring in soft tissues, recently described by WHO as a tumor of uncertain differentiation.
How is Chondrosarcoma treated?
Surgery is the main modality of treatment which is effective in Chondrosarcomas.
- ACT’s (Grade 1) of Extremities (long bones of limbs) can be at present safely treated with Extended curettage with or without adjuvants (phenol, liquid nitrogen) and filling of cavity with cement or bone graft.
The rates of local recurrence are low with this method of treatment for Grade I variant.
- The Surgical removal of the primary tumor with wide margins in the most optimal chance of cure in chondrosarcoma.
- Grade II, Grade III, and Peripheral, Dedifferentiated, Mesenchymal and Clear cell variants of chondrosarcoma are treated with Surgical excision with Wide margins.
All grades of chondrosarcoma in the pelvis and spine are termed as aggressive irrespectively and treated with Wide Excision.
Reconstruction of the defect can be done by any of the following methods:
- Tumor Prosthesis
- Biological Limb Salvage (Allograft or Recycled Tumor Bone)
- Graft prosthetic composite
- Rotationplasty
Rehabilitation also depends on the type of reconstruction.
Is there a role for chemotherapy or radiotherapy in chondrosarcoma?
- Chondrosarcoma is often regarded as resistant to both chemotherapy and radiotherapy.
- Newer studies have shown some improvement with chemotherapy and radiotherapy in mesenchymal type.
- In the dedifferentiated type, chemotherapy has a limited palliative role.
How often should one visit a doctor post treatment?
- The individual is followed up every 3 months for the first 2 years, followed by 6 months every 3 years (aggressive monitoring of the patient until 5 years).
- Later, one is seen every year for the next 10 years.
- The reason being that chondrosarcomas grow slow and are known to metastasize late.
- It is more common in lungs.
- Chondrosarcoma metastasis to bone is extremely rare.
- It is rare in grade I chondrosarcoma and clear cell chondrosarcoma, but 10 % of high grade variants of chondrosarcoma individuals present with lung metastases.
- This can be treated with surgical removal depending on the number and size of nodules in the lung.
- Metastases occurring during follow up will also be treated in the same manner.
- Local recurrences when identified should be treated with wide excision in high grade variants of chondrosarcoma.
- An aggressive approach provides a survival rate of 50-60 % at 10 years, which is better than osteosarcoma or chondrosarcoma.
- In contrast, local recurrences in grade I chondrosarcoma in long bones of limbs can be treated safely with extended curettage and does not affect survival.
1 Comment