
BIOPSY
This is almost always the final step to diagnose a bone or soft tissue tumor and not the first.
To achieve the best of outcomes, it is proposed to allow the final treating surgeon at a dedicated sarcoma center to perform the biopsy, irrespective whether the bone tumor is benign or malignant.
Always the tissue is accompanied by patient details, imaging films and reports which are sent to the pathologist to confirm the diagnosis.
Is a biopsy necessary?
- It is necessary to help diagnose certain infective and cancerous conditions.
- Majority of bone and soft tissue tumors undergo this as a confirmatory step.
What bone lesions do not need biopsy?
- Osteoid osteoma
- Osteochondroma
- Unicameral bone cyst
- Non-ossifying fibroma
- Ossifying fibroma
- Subcutaneous lipoma
- Intraosseous lipoma
How to prepare for a biopsy?
- Routine blood investigations such as complete blood profile, bleeding profile and serum calcium, phosphorous, alkaline phosphatase are performed.
- Plain radiographs, CT scan, MRI and bone scan or PET CT are performed as necessary.
- Informed consent of patient and relatives in native language is taken.
Where is biopsy obtained from?
- A successful biopsy is one where representative tissue is obtained in sufficient quantity.
- The clinical presentation and imaging modalities are taken into account to plan the site.
- The most reactive and solid portion of the growth is identified and approached.
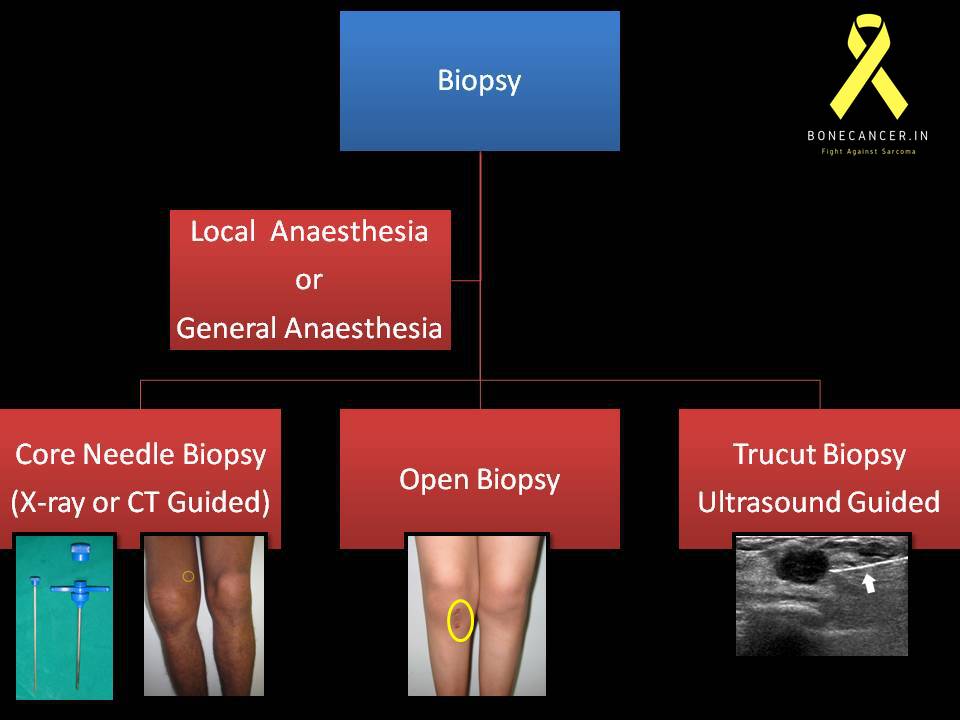
What method is used?
Different methods of biopsy are FNAC, Core biopsy (radio assisted or unassisted), Open biopsy, Gun Biopsy for soft tissue tumors.


- FNAC: Not routinely performed due to low yield.
- Fine needle aspiration cytology has the advantage of a very small incision, practically no risk of procedure or its complication.
- A 22-25 gauge needle is used which does not pose significant risk for tumor seeding.
- The disadvantages are that only cells can be obtained without matrix, usually done by a skilled cyto-pathologist, less accurate and invariably fails to lead to a diagnosis and requires a second core or open biopsy.
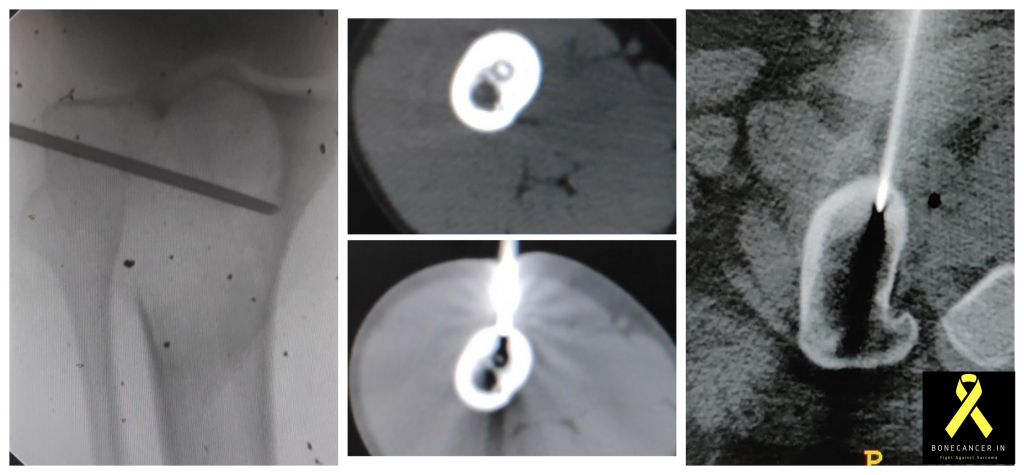
- CORE NEEDLE BIOPSY:
- This is the most common mode followed in dedicated bone tumor centers.
- A jamshidi needle is used, varying from 8G ~13G.
- It has a tapered distal tip and wider stem which does not crush the tissues.
- Image guided is the norm(Ultrasound or CT scan guided)
- The advantages are that there is a small surgical scar, short procedure time, can be performed on OPD basis or minimal sedation as in day care procedures, low cost and easily reproducible.
- Disadvantages are that a small area is sampled compared to open biopsy, the representative area may be missed if image guidance is not taken in some cases.
- OPEN BIOPSY:
- Certain bone tumors may require open biopsy, which can be the primary procedure or as secondary to confirm FNAC or Core needle.
- Incision is based on planned future surgery.
- It is best done in the specialist referral center rather than in a peripheral hospital
- A tourniquet is used almost always.
- Incision is longitudinal (not transverse) for most lesions in the extremity (except the pelvis and the scapula).
- Most direct route to the tumor is chosen so as to not contaminate tissue planes.
- Wound closure is water tight following biopsy.
- The bone defect is plugged with gel foam or bone cement to prevent bleeding into soft tissues.
- Meticulous hemostasis is achieved to prevent hematoma, otherwise may cause swelling, pain and discomfort.
- Suction drain tract is placed adjacent to and in line with the biopsy incision to evacuate hematoma.
- Open biopsy has certain advantages in that a large or sufficient sample is obtained for pathological diagnosis and grading may be more accurate.
- On the other hand, disadvantages are plenty such as invasive procedure, hospital stay, higher cost, anesthesia, not repeatable and a longer recovery time.
- FROZEN SECTION:
- In certain situations of ambiguity in diagnosis, like in case of differentiating a benign lesion from malignant during open biopsy or curettage surgery.
- This method is also utilized for confirmation of adequacy of resection margins (soft tissue or intra medullary resection).
- But frozen section has its limitations such as limited time and section for reporting.
Is Biopsy painful?
It is an invasive procedure. Adequate analgesia is used during the procedure.
- In case of core needle, the procedure is done on an outpatient basis or Operating room as required.
- Pain is less in Minimally invasive Procedures like Core Needle or TruCut.
- Adequate local anesthesia is provided in the form of lidocaine prior to biopsy. Oral analgesics for 3 days are sufficient to alleviate pain.
- The same is held for image assisted (CT or MRI assisted) biopsy.
- In case of open biopsy or inaccessible core needle biopsy, the procedure is carried out in the operating theatre and suitable analgesia is provided by the anesthetic
- Post procedure analgesics are provided via intravenous or oral route.
- The procedure is performed under appropriate empiric antibiotic cover.
- After discharge oral analgesics are to be continued for 5 days.
Can it be performed as Day-Care procedure?
- Yes, Image Guided Core needle and Trucut/Gun biopsy can be performed on a day care basis.
How long does it obtain report ?
- Usually it takes 3-4 days for report to be confirmed.
- In certain situations to confirm the etiology, the pathologist may perform immunohistochemistry tests on obtained tissue samples.
- This may prolong the reporting by 3-4 days.
- Certain tests like PCR or FISH may be needed to confirm diagnosis.
What are complications associated with procedure?
- Complications are rare in biopsy procedures.
- Chances of infection
- Bleeding
- Prolonged pain and swelling at the biopsy site
- Deep vein thrombosis
- Pathological fracture
- Allergic reactions related to drugs
What are the chances of Re-Biopsy?
- This is a remote possibility since all necessary steps will be taken as explained before performing
- In rare cases when the biopsied tissue sample is inadequate due to loss (previously done elsewhere) and re confirmation.
- The latter issue is dealt with by obtaining confirmation of tissue diagnosis if required from two or more separate pathologists and also sending the whole tissue sample to each pathologist in succession.
- The material thus obtained is usually processed immediately and the report is generated in 2 to 3 days.
If the report is consistent with the clinical and radiological diagnosis, the doctor will advise further investigations to look for spread of the cancer and then the treatment.
If the report does not match with the clinical and radiological diagnosis, the reports have to be reviewed.
A second opinion of the material may be sought.
This is the most critical step as the whole treatment and prognosis of the patient depends on the diagnosis.
6 Comments